The Role of Home Care in Public Health Outcomes
The Role of Home Care in Public Health Outcomes

Home care is defined as the delivery of health and personal support services in a patient’s own home, reducing reliance on hospitals and improving outcomes for vulnerable populations. The role of home care in public health extends well beyond individual patients. It functions as a population-level intervention, reducing emergency department visits, preventing avoidable hospitalizations, and supporting chronic disease management in community settings. Research published in JAMA Health Forum and JAMA Network Open confirms that structured home care programs, including Medicaid Home and Community-Based Services (HCBS) and hospital-at-home models, produce measurable reductions in acute care utilization. For healthcare professionals, policymakers, and caregivers, understanding this evidence is the foundation for designing systems that actually work.
How does home care reduce acute healthcare use and improve outcomes?
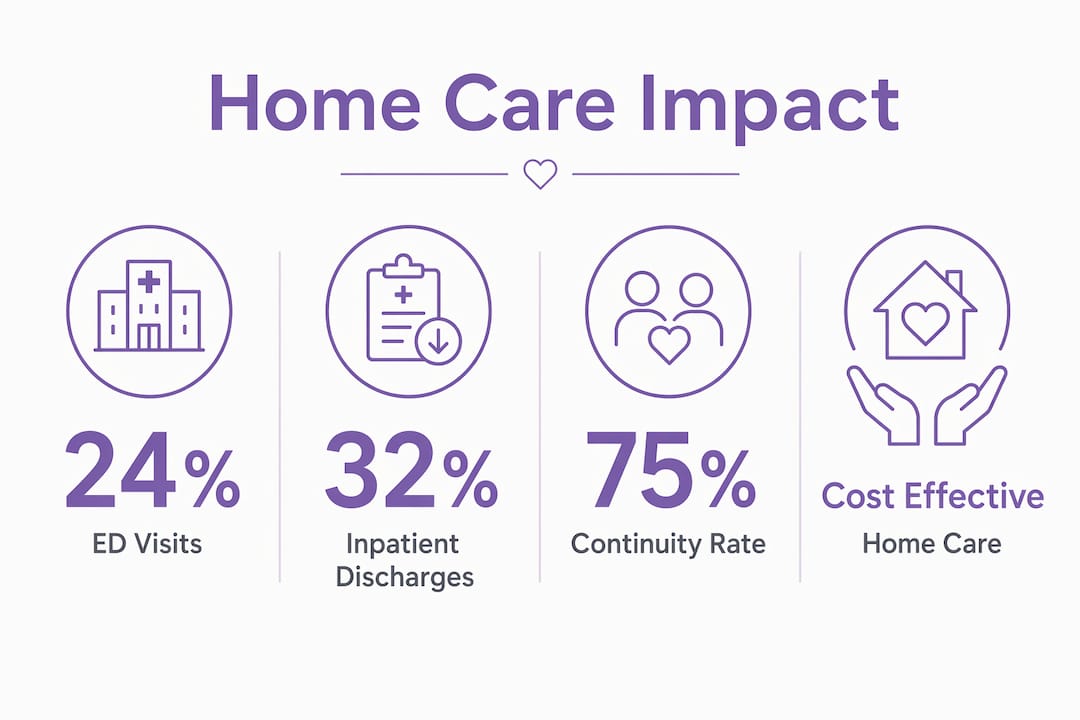
The mechanism is direct: home care replaces or prevents high-cost, high-risk acute care episodes by delivering monitoring, clinical support, and chronic disease management where patients already live. Medicaid HCBS initiation decreases emergency department use by 24% and inpatient discharge by 32% in a study of 1,218 older adults across 11 states. That reduction is not a one-time effect. The data shows persistent decreases in acute service use after HCBS enrollment begins, meaning the benefit compounds over time.
Hospital-at-home models produce even sharper results. In 15,871 Medicare beneficiaries, hospital-at-home mortality was 0.4% compared to 3.6% for traditional inpatient care. Thirty-day emergency visits were also lower: 8.8% versus 10.0%. Older adults face a disproportionate risk of hospital-associated complications, including infections, delirium, and falls. Removing them from the inpatient environment eliminates many of those risks entirely.
The mechanisms behind these outcomes include three core functions:
- Continuous monitoring of vital signs, medication adherence, and symptom changes before they escalate
- Support with activities of daily living, which prevents the functional decline that drives emergency visits in older adults
- Chronic disease management through structured protocols for conditions like heart failure, COPD, and diabetes
Pro Tip: When reviewing home care program data, look beyond readmission rates. Reductions in ED visits and inpatient discharges are stronger indicators of sustained public health impact than 30-day readmission figures alone.
The comparison with traditional inpatient care is not simply about cost. Home-based acute care preserves patient dignity, maintains family involvement, and reduces exposure to hospital-acquired conditions. For policymakers evaluating catastrophic care services and high-acuity home programs, these outcome differences justify significant investment in home-based infrastructure.
What types of home care services support community and individual health?
The Centers for Medicare and Medicaid Services (CMS) defines HCBS as person-centered care delivered in home and community settings that addresses functional limitations through both health and human services. That dual mandate is what separates effective home care from simple medical visits. CMS HCBS programs include skilled nursing, physical and occupational therapies, personal care assistance, transportation, homemaker services, counseling, and support for family caregivers through paid caregiver waivers.
This breadth matters because health outcomes are not determined by clinical care alone. A patient managing diabetes who cannot prepare meals, get to appointments, or maintain a clean living environment will deteriorate regardless of how skilled their nursing visits are. The integration of health and human services within a single care model is what produces the outcome reductions seen in JAMA research.
Key service categories within HCBS include:
- Skilled nursing and therapy: wound care, medication management, post-surgical recovery, physical and speech therapy
- Personal care assistance: bathing, dressing, mobility support, and toileting for individuals with functional limitations
- Homemaker and supportive services: meal preparation, light housekeeping, and errands that maintain safe home environments
- Transportation and care coordination: connecting patients to specialist appointments, community resources, and social services
- Culturally responsive care: services delivered in patients’ preferred language and aligned with cultural values, which improves engagement and adherence
HCBS programs typically cost less than residential care and provide familiar environments that patients prefer. That cost advantage, combined with superior outcomes, makes HCBS the most defensible model for policymakers allocating long-term care resources. Helping-hands-home-care delivers this integrated model directly, combining home health aide services with supportive personal care that addresses the full spectrum of patient need.
Why is continuity of care and workforce training critical in home care’s public health role?
Continuity of care is not a soft quality metric. It is a quantifiable driver of outcomes. A study of 1,207 patients published in the Annals of Family Medicine found that relational continuity at 75% or higher with GPs or nurses in home care settings reduces hospital admissions significantly, with odds ratios at or below 0.45. That means patients with stable, consistent care relationships are more than twice as likely to avoid hospitalization compared to those receiving fragmented care.

The practical implication is that ad hoc clinician switching blunts the public health gains from home care. When a different aide or nurse arrives at each visit, the relationship-based monitoring that catches early deterioration breaks down. Policymakers and care managers should treat assignment stability as a modifiable system variable, not an administrative inconvenience.
Workforce training is the second critical factor, and current policy falls short. A 2026 analysis published in BMC Palliative Care found that homecare worker training in end-of-life care lacks defined standards and role responsibilities in policy documents. Social homecare workers are under-recognized despite playing a direct role in patient safety and comfort during the final stages of life.
To address these gaps, healthcare systems and policymakers should:
- Establish minimum training standards for homecare workers covering symptom recognition, medication safety, and end-of-life communication
- Define role responsibilities clearly so workers understand the boundaries between personal care, clinical observation, and tasks requiring escalation
- Prioritize assignment consistency by building scheduling systems that maintain the same caregiver-patient pairings across visits
- Include homecare workers in care team communications, particularly for patients with complex or terminal conditions
- Fund ongoing education for caregivers managing patients with dementia, heart failure, or palliative care needs
Pro Tip: Continuity of care is a policy lever, not just a care quality goal. Scheduling systems that default to consistent assignments rather than available-slot filling produce measurable reductions in urgent care use without additional clinical resources.
The policy gaps in end-of-life homecare represent a systemic failure with direct public health consequences. Workers who lack training cannot identify deterioration, cannot communicate effectively with clinical teams, and cannot provide the consistent presence that keeps patients safely at home.
How do nurse-led community-based interventions enhance public health through home care?
Community-based nursing is the operational link between public health principles and home care delivery. A systematic review of 20 studies involving more than 14,000 participants confirmed that nurse-led home programs consistently improve health behaviors, quality of life, and reduce healthcare utilization. The effect is not marginal. It is consistent across geographies, patient populations, and care models when programs are locally adapted and well-structured.
The components that drive these results include:
- Home visits with structured assessment protocols that identify risk factors before they produce acute events
- Telehealth integration for between-visit monitoring of chronic conditions like hypertension, diabetes, and heart failure
- Patient and caregiver education on medication management, symptom recognition, and when to seek care
- Screening and prevention services delivered in the home, including fall risk assessments and cognitive screening
- Transitional care coordination by nurse case managers that reduces 30-day readmissions by bridging hospital-to-home gaps
Public health nursing operates on an upstream prevention model, addressing social determinants of health before they produce clinical crises. Home care is the delivery mechanism that makes this upstream work possible at scale. When a nurse visits a patient at home, she sees the refrigerator, the medication bottles, the fall hazards, and the social isolation that a clinic visit never reveals. That visibility is the public health advantage of home-based care.
Chronic disease self-management improves when patients receive education and support in their own environment. Guidance on chronic disease management consistently shows that adherence to treatment protocols increases when patients feel supported in familiar settings rather than managed in clinical ones. Nurse-led home programs align with the Chronic Care Model by activating patients, supporting self-management, and connecting individuals to community resources that sustain health between clinical contacts.
Key takeaways
Home care reduces acute healthcare utilization, improves population health outcomes, and functions as a cost-effective public health intervention when built on continuity, trained workforce, and integrated clinical and social supports.
| Point | Details |
|---|---|
| HCBS reduces acute care use | Medicaid HCBS initiation cuts ED visits by 24% and inpatient discharges by 32% in older adults. |
| Hospital-at-home lowers mortality | In-hospital mortality drops from 3.6% to 0.4% when acute care is delivered at home for Medicare patients. |
| Continuity drives outcomes | Relational continuity at 75% or higher with consistent caregivers reduces hospital admissions by more than half. |
| Workforce training gaps are a policy risk | Homecare workers lack defined training standards for end-of-life care, limiting safety and care quality. |
| Nurse-led programs improve population health | Systematic reviews of 14,000+ participants confirm nurse-led home interventions reduce utilization and improve quality of life. |
What I’ve learned about home care that most policy discussions miss
After years of working in and around home care, the pattern I keep seeing is this: the clinical evidence is strong, but the system design is weak. We have JAMA-level proof that home care reduces hospitalizations and mortality. We have CMS frameworks that define what integrated HCBS should look like. And yet, the actual delivery of care is still fragmented, inconsistent, and under-resourced in ways that prevent those outcomes from materializing at scale.
The continuity finding from the Annals of Family Medicine is the one that should be on every care manager’s wall. An odds ratio below 0.45 for hospital admissions is not a marginal improvement. It is a structural advantage that disappears the moment you rotate caregivers for scheduling convenience. The system optimizes for coverage, not relationships, and that choice has real consequences for patients.
The workforce training gap is the issue I find most frustrating. Social homecare workers are often the last professional contact a dying patient has. They are present for symptoms, for distress, for the moments that matter most. And yet, as the BMC Palliative Care analysis shows, policy documents provide almost no guidance on what those workers should know or do. That is not a minor oversight. It is a failure of the entire system to take home care seriously as a public health function.
My recommendation for policymakers is direct: stop treating home care as a cost-containment tool and start treating it as a public health infrastructure investment. That means funding training, mandating assignment consistency, and defining homecare worker roles with the same rigor applied to hospital staff. The evidence supports it. The gap is political will.
— Michael
How Helping Hands Home Care delivers evidence-based home care
The research is clear: home care works best when it combines skilled clinical support with consistent, person-centered personal care. Helping-hands-home-care provides exactly that model for elderly clients across the community.
Our home health aide services deliver the continuity and integrated support that the evidence shows reduces hospitalizations and improves quality of life. From personal care and daily living assistance to supportive services that keep clients safe and comfortable at home, Helping-hands-home-care builds the kind of consistent caregiver relationships that produce real health outcomes. We also offer massage therapy as part of our person-centered care approach. Contact us to learn how our services align with your care goals.
FAQ
What is the role of home care in public health?
Home care reduces emergency department visits, prevents avoidable hospitalizations, and supports chronic disease management in community settings. It functions as a population-level intervention by delivering clinical and personal support services where patients live.
How does home care improve health outcomes for older adults?
Medicaid HCBS initiation reduces ED use by 24% and inpatient discharges by 32%, while hospital-at-home models lower in-hospital mortality from 3.6% to 0.4% compared to traditional inpatient care.
Why does continuity of care matter in home-based settings?
Relational continuity at 75% or higher with consistent GPs or nurses reduces hospital admissions significantly, with odds ratios at or below 0.45. Caregiver switching disrupts the monitoring relationships that catch early deterioration.
What services are included in home and community-based services?
CMS defines HCBS to include skilled nursing, physical and occupational therapy, personal care assistance, homemaker services, transportation, and counseling. These services address both clinical needs and functional limitations that affect daily living.
What are the biggest gaps in home care workforce policy?
A 2026 BMC Palliative Care analysis found that homecare workers lack defined training standards and role responsibilities for end-of-life care. This policy gap limits care quality and safety for patients in the final stages of life.