Why Home Care Improves Recovery for Elderly Patients
Why Home Care Improves Recovery for Elderly Patients

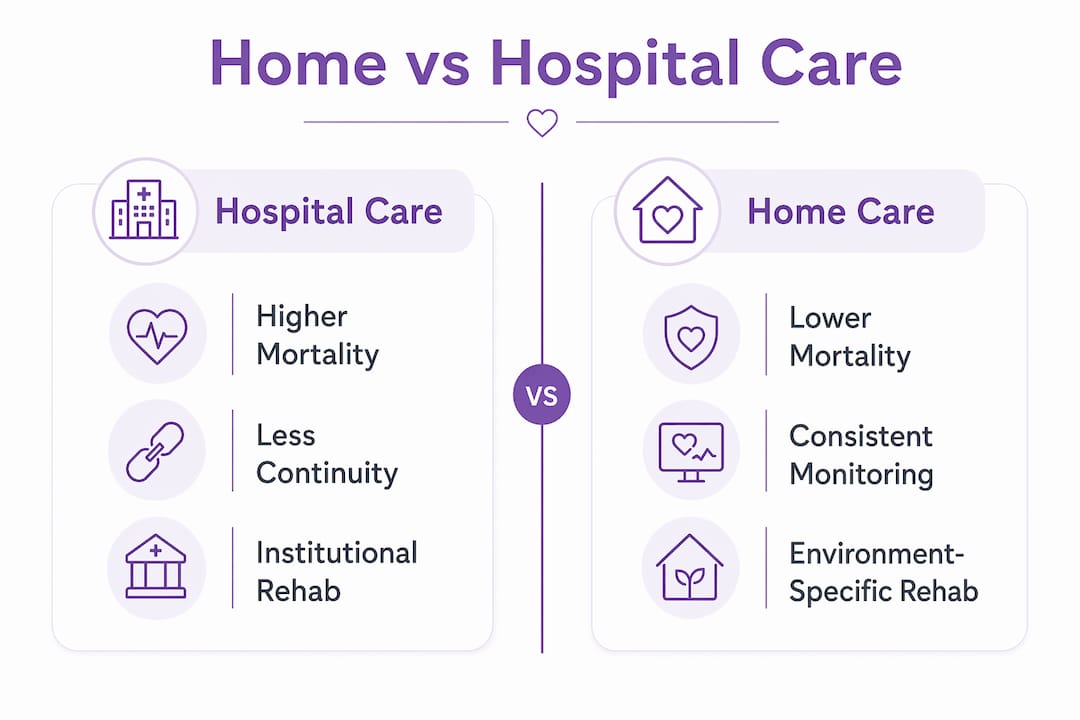
Home care improves recovery by delivering personalized clinical support, consistent monitoring, and emotional stability inside a patient’s own environment, where healing happens fastest. For families researching options for an elderly loved one, the evidence is no longer ambiguous. Studies from 2026 show that home-based care reduces hospital readmissions, lowers mortality rates, and cuts urgent care visits compared to traditional inpatient stays. The difference comes down to three factors: continuity of care, environment-specific rehabilitation, and structured clinical oversight. Understanding each one helps you make a better decision for your family member’s recovery.
Why home care improves recovery more than inpatient stays
The clinical case for home care over extended hospital stays is now backed by large-scale real-world data. A 2026 UK analysis of 2,905 hospital-at-home episodes found that bed-day savings exceeded 13,000 over 33 months, with meaningful reductions in 30-day readmission rates. That is not a marginal improvement. It represents thousands of patients who recovered at home without returning to the hospital within a month.
The mortality data is even more striking. A study of 15,871 Medicare beneficiaries showed that in-hospital mortality was 0.4% for hospital-at-home patients versus 3.6% for traditional inpatient care. That adjusted odds ratio of 0.09 means home care patients were roughly nine times less likely to die during their care episode. Emergency department visits within 30 days were also lower for the home care group.
The reason behind these numbers is early detection. Home-based clinical teams monitor patients daily in the environment where subtle changes, like reduced appetite, altered gait, or medication side effects, are easier to catch before they escalate. Hospitals, by contrast, are high-traffic environments where individual patient changes can go unnoticed until they become acute. You can review home care’s public health impact for a broader look at how these outcomes connect to population-level trends.

| Metric | Hospital care | Home-based care |
|---|---|---|
| In-hospital mortality rate | 3.6% | 0.4% |
| 30-day readmission trend | Higher | Reduced |
| Average bed-days used | Longer stays | Net savings of 3+ days |
| Emergency department visits (30-day) | More frequent | Lower adjusted odds |
Pro Tip: When evaluating a home care provider, ask specifically whether they have a clinical escalation protocol. A provider with a documented process for detecting and responding to deterioration is operating at a fundamentally different level than one offering basic caregiver presence.
How continuity of care shapes home recovery outcomes
Continuity of care is the biggest hidden variable in home recovery. A 2026 study published in the Annals of Family Medicine found that patients who received 75% or more of visits from the same GP or nurse had hazard ratios of 0.61 to 0.69 for urgent care use and hospital admissions. In plain terms, consistent provider assignment reduced the likelihood of an emergency visit by 30 to 40 percent.
Why does this matter so much? A clinician who sees the same patient repeatedly builds a baseline understanding of that person’s normal. They notice when something is off before it becomes a crisis. A rotating roster of unfamiliar caregivers, even skilled ones, lacks that reference point. Each handoff introduces a gap where critical information can fall through.
Here is what families should look for when selecting a home care provider with strong continuity:
- Assigned care team: Ask whether your loved one will have a primary nurse or aide who covers the majority of visits, not a pool of rotating staff.
- Documented care notes: Providers with structured visit documentation allow any clinician to review recent changes, reducing the risk of missed deterioration.
- Threshold tracking: The best programs track continuity percentages internally and flag cases where provider consistency drops below acceptable levels.
- Transition planning: Strong continuity extends through discharge. Ask how the provider coordinates with the hospital team during the handoff period.
Pro Tip: The first two to four weeks after hospital discharge are the highest-risk window. Prioritize providers who schedule their most experienced clinicians during this period, not just during the initial assessment.
Does home-based rehabilitation actually improve functional recovery?
The answer is yes, and the data from hip fracture patients makes the case clearly. A Norwegian registry analysis of patients aged 60 and older showed that home-based rehab mortality at one year was 7.7% compared to 15.9% for institutional rehabilitation. The 30-day readmission odds ratio for home care was 0.56, meaning home rehab patients were nearly half as likely to return to the hospital within a month.
The mechanism is straightforward. Practicing mobility in the actual environment where a patient lives produces better functional gains than practicing in a generic institutional setting. A person relearning to walk after a hip fracture needs to navigate their own hallway, their own bathroom threshold, and their own kitchen layout. Institutional rehab cannot replicate that specificity.
Families asking rehab providers the right questions will get better outcomes. Here is a practical checklist:
- Ask about home environment assessment. A qualified rehab provider will visit the home before or at the start of care to identify fall hazards, assess furniture height, and recommend grab bar placement.
- Ask about task-specific training. Therapy should include practice with the patient’s actual daily tasks: getting in and out of their specific bed, using their shower, climbing their front steps.
- Ask about family involvement. Effective home rehab programs train family members to support exercises between visits, not just observe them.
- Ask about progress benchmarks. Providers should set measurable functional goals and review them at defined intervals, not just continue visits indefinitely.
- Ask about coordination with the primary physician. Rehab gains are undermined when the therapy team and the prescribing doctor are not communicating about medication changes or pain management.
Environment-specific therapy is not a comfort preference. It is a clinical advantage that institutional settings structurally cannot replicate.
What makes a structured home care program clinically effective?
Not all home care is equal. The difference between a program that genuinely improves outcomes and one that simply provides companionship lies in its clinical architecture. The Thrive transitional care trial demonstrated this directly. The program increased home health referrals and produced lower 30-day readmissions and emergency visits compared to standard discharge. Fewer than 20% of Medicaid-insured patients currently receive home health referrals after hospitalization, which means most patients who would benefit are not getting access.
What separates a high-quality program from a basic one comes down to specific components:
- Medication reconciliation: The first week home is when medication errors peak. Structured programs include a pharmacist or nurse review of all prescriptions against the discharge summary to catch conflicts or missed doses.
- Interdisciplinary case conferencing: Effective programs hold regular team meetings where nurses, therapists, social workers, and physicians review each patient’s status together. This prevents siloed care where one provider is unaware of changes another has documented.
- Social work involvement: Vulnerable elderly patients often face housing instability, food insecurity, or caregiver burnout that directly affects recovery. Social workers embedded in home care programs identify and address these barriers before they derail clinical progress.
- Real-time escalation pathways: High-quality home care is protocolized. When a clinician detects a warning sign, there is a documented process for escalating to a physician or emergency services, not a judgment call made in isolation.
Families should ask any prospective provider to describe their escalation protocol and their interdisciplinary team structure. Providers who cannot answer those questions clearly are not operating at the clinical level that recovery demands. Exploring professional home care plan examples can help you understand what a well-structured care plan looks like in practice.
Key takeaways
Home care improves recovery because it combines consistent clinical monitoring, environment-specific rehabilitation, and structured interdisciplinary support in the setting where elderly patients are most stable and responsive to care.
| Point | Details |
|---|---|
| Mortality advantage is significant | Home-based care patients show 0.4% mortality vs 3.6% in traditional inpatient settings. |
| Continuity of care reduces emergencies | Patients with 75%+ same-provider visits have 30–40% lower urgent care and admission rates. |
| Home rehab cuts readmissions in half | Norwegian registry data shows home rehab patients have a 0.56 odds ratio for 30-day readmission. |
| Clinical structure determines outcomes | Programs with medication reconciliation, case conferencing, and escalation protocols produce measurably better results. |
| Most eligible patients are not referred | Fewer than 20% of Medicaid-insured patients receive home health referrals despite clear evidence of benefit. |
What families get wrong about home care quality
I have spent years reviewing how families approach home care decisions, and the most common mistake is treating it as a comfort choice rather than a clinical one. Families often assume that any warm, attentive caregiver will produce good recovery outcomes. The research says otherwise. The gap between a provider with documented escalation protocols and one without is not a quality-of-life difference. It is a mortality difference.
The second mistake is undervaluing continuity. Families sometimes accept rotating staff because it seems more flexible or because the agency presents it as normal. It is not optimal. The Annals of Family Medicine data makes clear that relational continuity with assigned clinicians is measurable and directly tied to fewer hospitalizations. When you are evaluating providers, ask for their staff assignment policy in writing.
The third thing I would push back on is the assumption that home care is only appropriate for patients who are already stable. The 2026 hospital-at-home data shows that patients receiving acute-level care at home had dramatically better outcomes than those in traditional inpatient settings. Home care is not a step-down option. For many elderly patients, it is the superior clinical choice from the start.
What I tell families is this: treat the selection of a home care provider with the same rigor you would apply to selecting a surgeon. Ask about credentials, protocols, and outcomes. The providers who welcome those questions are the ones worth trusting.
— Michael
How Helping-hands-home-care supports your family member’s recovery
Helping-hands-home-care provides professional home health aid services designed specifically for elderly recovery, with assigned caregivers who build the consistent relationships that the research shows matter most. Every care plan is built around the individual patient’s home environment, daily routines, and clinical needs, not a generic template. Beyond direct care, Helping-hands-home-care also offers house cleaning services to maintain a safe and hygienic recovery environment, and massage therapy to support pain relief and mobility as part of a broader recovery plan. Explore the full range of home care services and find the right combination of support for your loved one’s recovery at home.
FAQ
Why does home care reduce hospital readmissions?
Home care reduces readmissions by providing daily clinical monitoring that catches complications before they require emergency intervention. Studies show structured home care programs lower 30-day readmission rates compared to standard discharge without follow-up support.
What is continuity of care and why does it matter for recovery?
Continuity of care means receiving the majority of visits from the same assigned clinician rather than rotating staff. Research shows patients with 75% or more visit continuity have significantly lower rates of urgent care use and hospital admissions during recovery.
Is home-based rehabilitation as effective as institutional rehab?
Home-based rehabilitation produces better outcomes for many elderly patients, particularly after hip fracture. Norwegian registry data shows one-year mortality of 7.7% for home rehab versus 15.9% for institutional rehab, with lower 30-day readmission rates as well.
What should I look for in a home care provider for an elderly parent?
Look for providers with assigned care teams, documented escalation protocols, medication reconciliation processes, and interdisciplinary coordination between nurses, therapists, and physicians. Providers who cannot describe these systems clearly are not operating at the clinical level recovery requires.
How soon after hospital discharge should home care begin?
Home care should begin as close to discharge as possible. The first two to four weeks post-discharge are the highest-risk period for complications and readmission, making early clinical monitoring the most time-sensitive component of a successful recovery plan.